If your neck tension keeps coming back, your knee takes load it was not built to carry, or your glutes will not show up no matter how much you train, you are not dealing with separate problems. You are dealing with one pattern. And it almost never starts where you feel it.
You have jaw tension. Or a knee that absorbs what the foot will not. Or glutes that have been activated, cued, and trained. Still not showing up.
None of those are where the pattern started.
And in many cases, they are not where it is being driven from either.
In 23 years of clinical practice, I have assessed thousands of compensation patterns. The foot grip is present in almost all of them. Not because the foot is the problem, but because the foot stopped being trusted. The system adapted to that loss of trust, and everything above reorganized to manage it.
One pattern. Different addresses.
This is what I see every week in my Wicker Park studio in Chicago, and it is almost never where people expect it to start.
This is what that reorganization actually looks like.
A Little Anatomy First
Your foot contains 26 bones, 33 joints, and more than 100 muscles, tendons, and ligaments. That is not excess structure. It is a precision sensory platform.
The plantar surface of your foot is one of the most mechanoreceptor-dense areas in your body, outside of your hands and face.
Four receptor types are constantly feeding information upward:
Meissner’s corpuscles respond to light touch and surface contact.
Pacinian corpuscles detect vibration and deep pressure. Your high-speed positional reporters.
Ruffini endings respond to sustained stretch and are directly linked to nervous system downregulation.
Merkel discs track precise, sustained pressure and fine surface detail.
If you have ever sprained the same ankle more than once, worn a brace for an extended period, or broken a toe, your proprioceptive signal at ground level was already altered. The receptors in that tissue are not what they were. The brain has been compensating for that gap ever since, and the pattern above it reflects that.
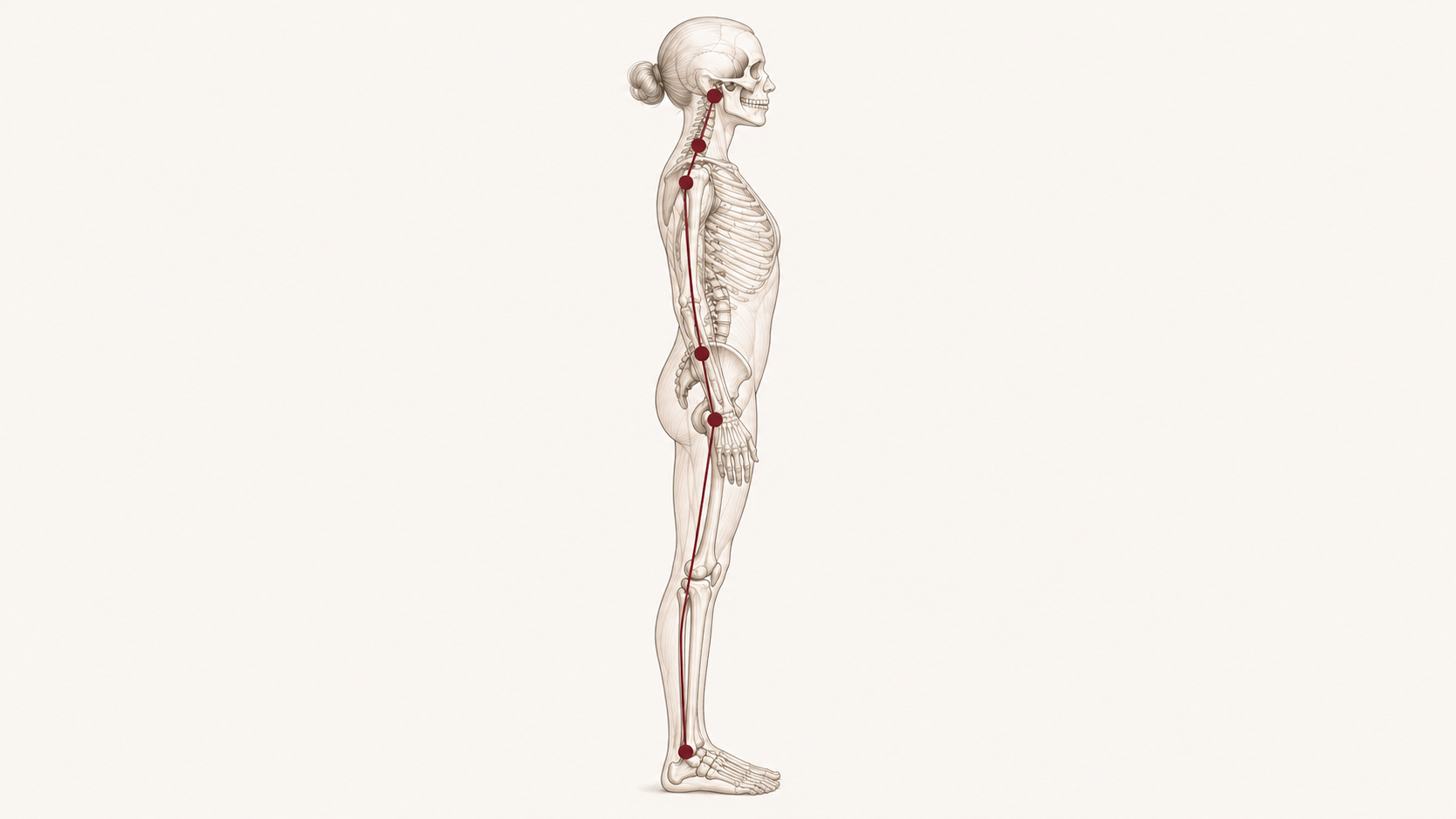
Every step sends positional data through your spinal cord to the cerebellum, vestibular system, and sensorimotor cortex. Your brain uses that information to organize posture, coordinate movement, and distribute load through every structure above.
When that input is compressed by narrow shoes, chronic tension, or years of compensation, the brain does not adapt well without it. It reorganizes.
And that reorganization moves up the chain in a very predictable sequence.
Why Does My Knee Hurt When My Foot Feels Fine?
When the foot grips, the intrinsic muscles stay in low-grade contraction. The toes compress. The big toe loses its ability to abduct. The foot loses its ability to move through a full range of pronation and supination.
That loss does not stay local.
The ankle joint contains some of the highest concentrations of joint mechanoreceptors in the body. When that input is degraded by chronic grip and compression, the knee does not just absorb torsional load. It also loses the positional data it needs to track accurately.
The joint is not unstable. It is uninformed.
Joint mobility is not just about range of movement. It is about the quality of the sensory information the joint produces as it moves through that range. When mechanoreceptor density is reduced by chronic compression or old injury, the joint loses its ability to report its own position accurately. Mobility without accurate proprioceptive feedback is movement without a map. The nervous system responds by restricting range to stay within what it can track. Restoring the input restores the access. That is why joint mobility improves when the proprioceptive environment improves, not because the joint changed, but because the nervous system finally has the information it needs to allow the movement.
The knee is a hinge. It is not designed to manage rotation.
When the foot cannot absorb and organize rotation at ground level, the tibia compensates. The knee begins to take on torsional forces it was never built to handle. Over time that shows up as tracking issues, medial knee pain, and patellofemoral compression.
When the arch collapses under a grip pattern, the femur internally rotates. That drives knee valgus. What most people call a weak knee problem is often a foot input problem the knee is expressing.
The knee is compensating for the foot.
Why Won’t My Glutes Fire No Matter How Much I Train?
This is where most people lose the thread.
Glute max does not fire in isolation. It fires as part of a coordinated sequence that begins with ground contact.
When the foot meets the ground, sensory input triggers a response through the posterior chain: foot, tibialis posterior, glute max, contralateral latissimus dorsi. That is the deep longitudinal subsystem firing in the sequence it was designed for.
When the foot is gripping, that sequence breaks at step one.
A distorted ground signal is read by the brain as instability. The response is to brace the hip flexors.
When the hip flexor braces, the nervous system inhibits glute max on that side. This is reciprocal inhibition. The brain will not allow full hip extension when it does not trust the base below.
This is why glute work often does not transfer.
The issue is not effort. It is input.
You cannot train your way out of a pattern the nervous system is still protecting.
A Note for People Who Work With Their Hands
Musicians, dentists, surgeons, manual therapists, anyone whose livelihood depends on fine motor precision, are often the last people who connect their hand and forearm problems to what is happening below the ankle.
Grip is a whole-body pattern.
The foot grips at ground level for the same neurological reason the hand overtightens on an instrument or a handpiece. The nervous system is bracing because the foundation is not clear. When the brain does not trust what is happening below, it raises whole-body bracing tone. The hands are downstream of that decision.
This is why musicians with no hand injury develop forearm tendinopathies. Why dentists develop shoulder and neck compression that does not resolve with stretching. Why the harder they work on the upper extremity, the less it holds.
Nobody looked below the ankle.
Why Grip Asymmetry Matters
When the foot begins sending a reliable signal, the baseline bracing tone drops across the entire system. The hands do not have to work as hard to maintain precision. Fine motor endurance improves. Recovery between sessions improves. The grip reflex becomes a choice again instead of a default.
This is not about relaxing your grip. It is about giving the nervous system a reason to.
You do not need to be a musician or a dentist to feel this. Notice right now how hard you are holding whatever is in your hand. Your phone. Your coffee. Your pen.
Most people are gripping at three times the force the task actually requires.
That is not a hand habit. That is baseline bracing tone, a grip pattern, expressing in the most available place.
When the foot begins sending a reliable signal, that baseline drops. The grip softens without you deciding to soften it.
Not because you relaxed.
Because the nervous system finally had a reason to.
If one hand is gripping harder than the other right now, that asymmetry is information. It is the same side-to-side bracing pattern that shows up in the foot, the hip, and the jaw. The nervous system does not grip randomly. It grips where it feels least supported. The side gripping harder is the side your nervous system is asking to compensate for what is not holding below it. That compensation has a cost: reduced fine motor precision, faster fatigue, and a bracing pattern that does not turn off between tasks.
Why the Breath Is Part of the Same Pattern
Shallow breathing is not the problem. It is the system protecting a foundation it does not trust.
If you are not breathing deeply enough for your body to feel stable, that is not a breathing problem. It is a signal problem. The diaphragm, pelvic floor, and deep spinal stabilizers fire together as a pressure system that tells the nervous system the foundation is secure. When the foot is gripping and the proprioceptive signal is degraded, that pressure system cannot fully engage. The nervous system responds by bracing the superficial muscles instead: the jaw, the SCM, the hip flexors, the hands. Shallow breathing is the result of that bracing pattern, not the cause of it. This is why breathing exercises give temporary relief but do not hold. You cannot breathe your way into stability until the nervous system has the ground-level input it needs to allow the diaphragm its full range. Restore the signal. The breath follows.
 This pattern is not built in the gym. It is built and maintained by the accumulated repetitions of daily life. Every time you lift a bag, twist to reach the back seat, carry groceries, or stand at a counter for an hour, your nervous system runs whatever pattern it has available. Those are not neutral movements. They are loaded repetitions of the compensation your body has already organized around. Training adds load on top of that. A stronger muscle running the wrong pattern is a more efficient compensation, not a resolved one. That is not a failure of effort. It is a gap in the information the nervous system was working with. Fill the gap and the pattern has a reason to change.
This pattern is not built in the gym. It is built and maintained by the accumulated repetitions of daily life. Every time you lift a bag, twist to reach the back seat, carry groceries, or stand at a counter for an hour, your nervous system runs whatever pattern it has available. Those are not neutral movements. They are loaded repetitions of the compensation your body has already organized around. Training adds load on top of that. A stronger muscle running the wrong pattern is a more efficient compensation, not a resolved one. That is not a failure of effort. It is a gap in the information the nervous system was working with. Fill the gap and the pattern has a reason to change.
There is one more daily life moment worth naming. When you lift something over 20 pounds your body reflexively uses the breath to stabilize. The diaphragm descends, the pelvic floor braces, and the deep spinal stabilizers co-contract to create a pressurized cylinder around your spine. That is your built-in stabilization system doing exactly what it was designed to do.
But if the diaphragm is already being used as a postural brace, which happens when the foot grip pattern is present and the deep stabilizers stop coordinating, it cannot also pressurize on demand for the lift. The cylinder is already compromised before the object leaves the ground. The body recruits the superficial muscles instead. The erector spinae. The quadratus lumborum. The SCM. The upper trapezius.
This is why lifting something heavy feels like work in your neck and upper back rather than your core. The load went to the wrong muscles because the right system was already occupied before the lift began. That is not a technique problem. That is a stabilization system running on partial capacity before the lift began.
That click you hear when you lift your leg out to the side or shift your weight is information. The IT band and TFL snapping over the greater trochanter is not a structural problem. It is a load problem. When glute max and glute medius are inhibited, because the foot is not sending a clear signal and the hip flexors are bracing, the TFL takes over the stabilization job. The click is what happens when a structure built for movement is pressed into stability work it was not designed for. The same pattern this blog has been describing. Different expression. Same source.
The click closer to the SI joint is a different signal from the same pattern. When glute max is inhibited on one side, the SI joint loses its primary stabilizer. The ligaments compensate. The click is the joint moving through a small range the ligaments were not designed to manage. It is not the joint breaking down. It is the joint waiting for the muscle that is supposed to be doing that job to come back online.
The Pattern Moves Upward
The deep click or snap in the front of the hip during movement is the psoas. When the foot grip pattern is present and the hip flexors brace to compensate, the psoas shortens and tightens. The snap on hip flexion or rotation is the tendon sliding over the bony landmark it was never meant to load repeatedly. Same pattern. Different address.
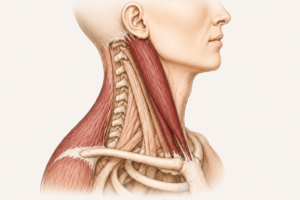
The click you hear when you rotate your neck, especially to one side more than the other, is the cervical joints or surrounding fascia moving under asymmetrical load. When the deep cervical stabilizers are inhibited and the SCM is overworking, the superficial structures slide over bony prominences they are not designed to contact. The side that clicks more is almost always the side the system has been asking to compensate longer.
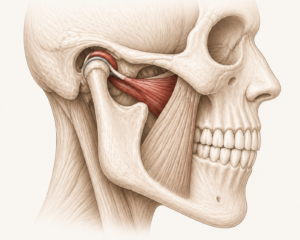 The jaw click is the articular disc. When the muscles surrounding the TMJ are under chronic tension, the lateral pterygoid pulling the disc forward, the click is the condyle sliding back under the disc on opening. It is not the joint deteriorating. It is the disc being asked to manage a load the surrounding musculature was supposed to share.
The jaw click is the articular disc. When the muscles surrounding the TMJ are under chronic tension, the lateral pterygoid pulling the disc forward, the click is the condyle sliding back under the disc on opening. It is not the joint deteriorating. It is the disc being asked to manage a load the surrounding musculature was supposed to share.
All five clicks. Different locations. One pattern running from the ground up.
What TCM Recognized Long Before the Research
Different systems. Same observation.
Traditional Chinese Medicine mapped the foot as a system gateway long before Western neuroscience had the tools to explain why.
The Kidney meridian, the only meridian that originates on the sole of the foot, begins at Kidney 1, Yongquan, or Bubbling Spring. Located at the anterior third of the plantar surface, it is considered the point where Earth energy enters the body.
In clinical TCM, stimulating K1 is used to ground the nervous system and address upward-rising patterns: jaw tension, occipital pressure, tinnitus, sleep disruption.
Beyond the Kidney meridian, the Liver, Spleen, Stomach, Bladder, and Gallbladder meridians all pass through the foot and toes. The big toe, where the Liver and Spleen meridians run, is directly implicated in patterns of pelvic and diaphragmatic tension. When the big toe cannot abduct freely, those pathways are functionally compressed.
Toe separators, from a TCM lens, are not stretching toes. They are restoring flow through gateways that govern structural stability and nervous system tone.
The mechanism is different from the Western model. The clinical observation is the same.
What Ayurveda Recognized
In Ayurvedic medicine, the feet are governed by Apana Vata, the downward-moving energy responsible for grounding, elimination, and structural stability. When Apana Vata is disrupted, the energy moves upward.
The presentation: anxiety, shallow breathing, jaw clenching, pelvic floor holding, poor sleep.
The foot marma point, Talahridaya, at the center of the sole, is a direct access site for restoring downward energy flow and calming the nervous system. Padabhyanga, therapeutic foot massage with warm oil, is prescribed specifically for Vata dysregulation, which maps closely to sympathetic nervous system overdrive in modern clinical terms.
Compression sleeves providing sustained, even pressure to the ankle and lower foot are doing mechanically what Padabhyanga does manually: activating Ruffini endings in a sustained pattern that signals safety to the nervous system.
The framework is different. The receptor response is the same.
How the Nervous System Responds to Consistency
Your brain maps your body based on the input it receives.
The more sensory input a region sends, the more cortical space it occupies. This is the cortical homunculus. In most modern adults, the foot’s representation is significantly smaller than it should be.
Years of shoes, flat surfaces, and reduced variability decrease the afferent signal from the foot. The brain’s map of the foot shrinks. When the map shrinks, the brain stops trusting the foot as a reliable anchor and begins bracing higher up the chain.
Hip flexors tighten. The jaw engages. The suboccipitals hold. The diaphragm loses range.
The glutes go quiet because the foundation they depend on is no longer sending a clear signal.
This is not dysfunction. This is adaptation.
Neuroplastic change, actual cortical remapping, requires repeated reliable input over time. That is where these tools come in.
Do Toe Separators Actually Work?
They Don’t Fix the Foot. They Change the Signal.
Toe separators and compression sleeves are not corrective devices. They do not fix the foot.
What they do is create the sensory conditions under which the nervous system can let go of a grip pattern it adopted for a reason.
Toe separators restore the spacing necessary for abductor hallucis to actually function. When that muscle engages, it activates proprioceptive loops that feed directly into the cerebellum. The cerebellum uses that input to begin reorganizing postural tone from the ground up.
Start seated or supine for 20 to 30 minutes. The foot needs to own the new spacing before it can use it under load.
Compression sleeves provide consistent mechanoreceptor activation at one of the highest-priority proprioceptive zones in the body. Worn during light movement or your morning routine, they help the brain locate the ankle with greater precision without demanding effort.
There is another layer.
The foot is a primary lymphatic return site. The plantar pump, the pressure differential created by normal foot loading, drives lymphatic fluid back up through the lower extremity. When the foot grips and loading patterns compress rather than mobilize, that pump underperforms. Fluid pools. Tissue becomes dense.
Consistent compression supports that return. Not as a treatment, but as a circulatory assist within a system that is already trying to move.
Andrew Taylor Still, the founder of osteopathy, observed over a century ago that when fluid flow is obstructed by tissue compression, the body cannot perform its basic physiologic functions. The plantar pump and the diaphragmatic pump are two of the mechanisms he was describing. This is not new science. It is foundational science that modern neuromuscular work is finally catching up to.
Sequencing matters.
Toe separators first.
Breathing next.
Movement after.
The sleeve stays on through all of it.
This is also where we layer in Align and Breathe. Low-effort, repeated input paired with breathing gives the nervous system a different option. One it can repeat. One it can keep.
Not as a separate routine. As part of your day.
The nervous system does not reorganize around novelty. It reorganizes around consistency.
One More Thing
Pain is not the warning.
Pain is what happens when the warning was missed.
Your body has been signaling all along.
The cues you received were not wrong.
Your body responded the only way it could with the input it had. The glute knows how to fire. The brain inhibited it because the base did not feel reliable.
That is not failure. That is protection.
And releasing the foot alone is not the answer.
Massage, rolling, stretching, all useful inputs. But one input does not reorganize a compensated ecosystem.
The foot is connected to the knee, the hip flexor, the pelvic floor, the jaw. One point addressed in isolation gives you temporary change. The pattern addressed as a system gives you a different nervous system response.
One that holds.
Can an Old Ankle Sprain Cause Problems Years Later?
If you are dealing with:
- Knee tracking issues or medial knee pain
- Glutes that do not fire despite consistent training
- Jaw tension or tinnitus
- Suboccipital pressure or cervicogenic headaches
- Pelvic floor holding
- Poor sleep or difficulty downregulating
Your foot may not be the origin of the symptom.
But it is almost certainly part of the pattern maintaining it.
If any of these are also true: you have sprained the same ankle more than once, spent months in a brace, or broken a toe that was never retrained, the signal disruption started earlier than you think.
The foot is the first input in the proprioceptive chain. When that input is compromised, every structure above compensates. When you restore it, consistently not occasionally, the chain has the information it needs to reorganize.
The system is designed to resolve. Sometimes it needs help identifying what it is still protecting against.
You are not rebuilding from broken.
You are building on what your body already knows.
Adapted is not damaged.
Your body adapted. It did not fail.
Frequently Asked Questions
Is this relevant if I do not have foot pain?
Yes. The foot grip pattern is a neurological adaptation not a pain condition. Most people with this pattern have no foot pain at all. The symptoms show up higher in the chain: knees, hips, jaw, suboccipitals, which is exactly why nobody connects them back to the foot.
How is this different from a podiatrist or PT assessment?
Podiatry addresses foot structure. Physical therapy addresses movement patterns. Neuromuscular assessment addresses the compensation chain: what the nervous system is protecting and why, from the ground up. The distinction is not about who is better. It is about which question is being asked.
Can I address this on my own?
The stacking assisted inputs in this post are a starting point. Toe separators and compression sleeves restore sensory conditions. A full assessment maps your specific pattern so the inputs are sequenced correctly for your body rather than applied generally.
Do you see clients in person in Chicago?
Yes. In-studio Discovery Sessions are available at the Wicker Park studio in Chicago. $250 for 45 minutes. Virtual sessions are also available nationwide at $145. Both begin with a full neuromuscular assessment before any hands-on work.
How long does it take to see a change?
That depends on how long the pattern has been running and what is maintaining it. Most clients notice a shift in their first session because the assessment itself changes what the nervous system is being asked to do. Lasting change requires consistent input over time. That is what the stacking tools and Align and Breathe protocol are designed to support between sessions.
Ready to Understand Your Specific Pattern?
If you see yourself in this pattern, the next step is not more exercises.
It is seeing how your system is actually organizing.
That is what we do in a Discovery Session.
Chicago clients: in-studio sessions are available this week in Wicker Park. $250.
Virtual sessions are available nationwide. 45 minutes. $145.
Not sure where to start:
Take the quiz: maranicandronmtappointments.com/quiz
Mara Nicandro, BCTMB
NMTForHealth Chicago
{kind=link}